
You made it through the day. Barely. By 3pm, the burning under the front of your foot was bad enough that you were walking differently — shifting weight to your heel, taking shorter steps, doing that thing where you count down the minutes until you can sit down. You took off your shoes the second you got home and pressed your fingers into the ball of your foot and thought: what is happening in there?
Here’s what’s probably happening: your shoes are doing something your feet were never designed to handle. Not because the shoes are cheap. Not because you’re doing anything wrong. But because the ball of your foot — that padded area just behind your toes — absorbs an enormous amount of force with every single step, and when the shoe underneath it isn’t built correctly for your foot, that force has nowhere to go except into your joints and nerves.
This guide will explain why the ball of your foot hurts, how to figure out which cause applies to you, and — crucially — what to actually do about it, starting with the shoe you’re wearing right now.
Key Takeaways
- The ball of your foot bears up to 2–3 times your body weight with every walking step, and significantly more during running or going down stairs.
- The most common and most overlooked cause of ball-of-foot pain is shoe structure — specifically, shoes that flex at the wrong point or lack metatarsal support.
- Pain in the ball of the foot has a clinical name — metatarsalgia — and while it sounds serious, most cases respond well to shoe changes before any medical treatment is needed.
- Women are significantly more affected than men, largely due to narrower toe boxes and heel elevation in common footwear styles.
- If pain has persisted for more than two to three weeks despite shoe changes, or if you feel numbness or shooting pain between your toes, it’s time to see a podiatrist.
What’s Actually Happening Inside Your Foot
Before getting into causes and fixes, it helps to understand what’s going on anatomically — not in a textbook way, but in a “this will actually help you buy the right shoe” way.
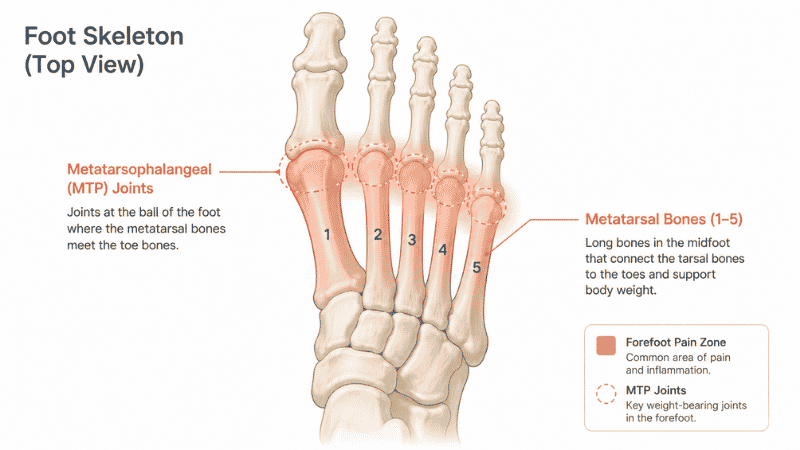
The ball of your foot is the area between the arch and the toes. Underneath the skin and padding, there are five long bones called metatarsals that fan out from your arch to the base of each toe. Where each metatarsal meets the toe is a joint — the metatarsophalangeal (MTP) joint. These joints are surrounded by nerves, tendons, small fluid-filled sacs called bursae, and a thick pad of fatty tissue that acts as a natural shock absorber.
Every time you take a step, your weight rolls forward through the heel, through the arch, and then pivots off the ball of your foot before your toes push off the ground. That pivot point — the ball — is where your foot experiences peak pressure. Research published in Foot & Ankle International found that forefoot loading during normal walking can reach 1.2 to 1.5 times body weight, and during running, that figure climbs considerably higher.
The system works beautifully when everything is aligned. When it doesn’t — because of a shoe that bends in the wrong place, a structural imbalance in your foot, or simply too many hours on hard floors — the metatarsal joints get overloaded, and that’s when the burning, aching, and sharp pain under the front of your foot begins.
Quick Self-Check: Which Type of Ball-of-Foot Pain Do You Have?
Not all forefoot pain is the same, and the fix depends on which category fits you. Spend 60 seconds with this.
The burning/aching after long periods of standing — worse at the end of the day, better after rest. Usually diffuse across the whole ball of the foot. This is classic metatarsalgia from overload — almost always shoe-related.
Sharp pain between your third and fourth toes that feels like a pebble in your shoe or an electric shock when you squeeze the front of the foot. This is more likely Morton’s neuroma — a thickened nerve that gets compressed by narrow shoes. Needs different attention.
Pain under one specific spot, usually the second metatarsal head, that’s tender when you press directly on it. Often seen in people with a longer second toe or high arches. This is a stress-related metatarsal issue and can worsen quickly with continued high-impact activity.
General forefoot soreness with stiffness in the big toe joint, especially in the morning. This pattern can indicate turf toe or early arthritis in the first MTP joint — worth getting evaluated.
If you’re in the first category — diffuse burning and aching, worse after standing or walking — read the whole guide. That’s what this article is built around, and it’s what shoe changes can genuinely fix.
Why Does the Ball of My Foot Hurt? The Six Most Common Causes
1. Your Shoe Bends in the Wrong Place
This is the most common cause of ball-of-foot pain that nobody talks about, and it’s entirely fixable with the right shoe.
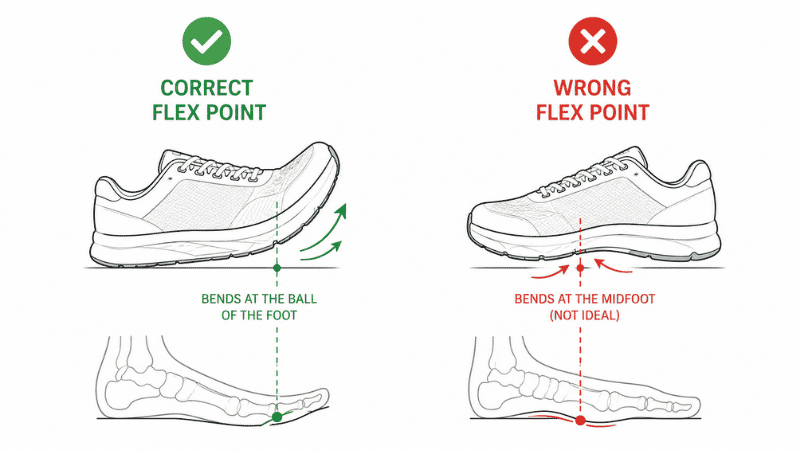
Every shoe has a flex point — the place where it bends when you walk. Shoes are engineered (or should be) to flex at the ball of the foot, which is where your foot naturally pivots during a step. When the flex point is too far forward — under the toes — or too far back — under the arch — your foot has to work against the shoe rather than with it. The metatarsal joints absorb that mismatch with every step.
Here’s a quick test: hold your shoe at the heel and press down on the toe. Watch where it bends. It should fold roughly at the ball — the widest part, about a third of the way from the front. If it bends near the middle or resists bending entirely, it’s working against your foot’s natural motion.
The fix: Look for shoes with a defined flex point at the forefoot. Running shoes and walking shoes from reputable athletic brands generally do this well. Dress shoes and fashion sneakers — even expensive ones — often fail this test completely.
2. There’s Not Enough Metatarsal Support
Your foot has a transverse arch — a subtle curve that runs across the width of the foot, not just lengthwise. Most people have heard of arch support meaning the longitudinal arch (the one on the inner side of your foot), but the transverse arch across the metatarsal heads is equally important and almost universally ignored by shoe manufacturers.
Without support under the metatarsal heads, those five bones splay apart and drop under load, increasing the surface area hitting the ground with every step and reducing the foot’s ability to distribute pressure evenly. The result is concentrated stress on whichever metatarsal is bearing the most load — and that’s where the pain develops.
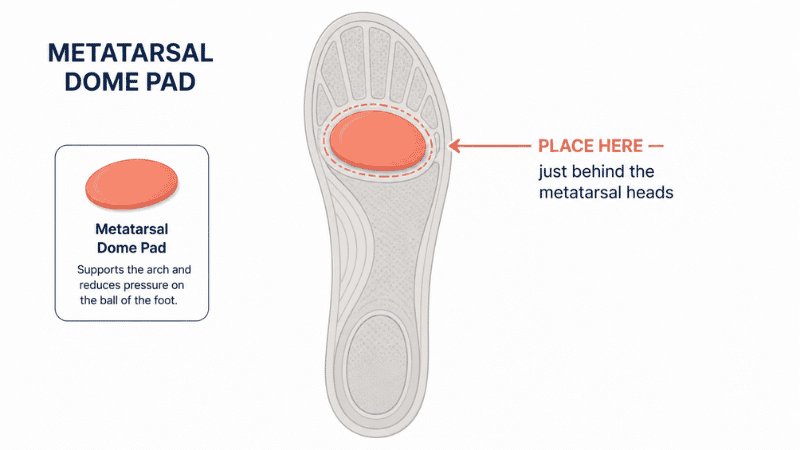
The fix: Look for shoes with a metatarsal pad or metatarsal bar — a raised ridge just behind the metatarsal heads. Alternatively, aftermarket insoles with a metatarsal dome (Superfeet and Powerstep both make good options) can add this support to shoes you already own. This is often the single most effective intervention for diffuse forefoot pain.
3. Your Shoes Are Too Narrow at the Toe Box
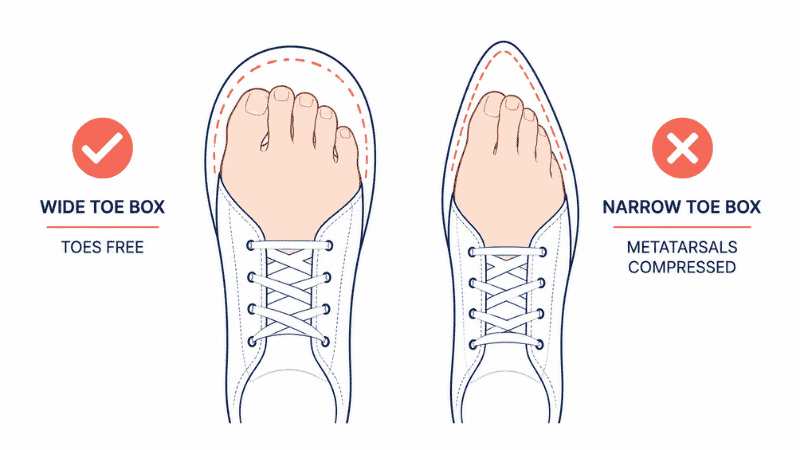
This one affects women disproportionately. The standard pointed or tapered toe box in most women’s dress shoes, fashion sneakers, and even some athletic shoes compresses the metatarsal heads together. When those joints are forced inward against each other over hours of wear, the bursae become inflamed, the nerves get irritated, and the whole forefoot becomes tender.
The insidious part is that the shoe might feel fine for the first hour — the compression is gradual, and your foot doesn’t fully protest until it’s been squashed for a while. By the time you notice the pain, the irritation is already significant.
The fix: The toe box should be wide enough that you can wiggle all five toes without any of them pressing against the sides. When you’re in the store, press your thumb on the outer edge of the shoe at the widest toe — there should be a slight give, not immediate resistance. Brands with consistently wider toe boxes for women: Altra, Hoka, New Balance in wide sizes, and Brooks. For men, New Balance and Brooks are reliable.
4. Your Heel Is Elevated — Even Slightly
Most people associate heel pain with high heels. But any heel elevation — even the modest 8–12mm heel-to-toe drop in standard running shoes — shifts body weight forward onto the forefoot. If you’re wearing shoes with a significant heel lift for most of your waking hours, you’re spending most of your day with your metatarsals under elevated load.
This matters most for people who stand on hard floors for long shifts — think retail workers, teachers, healthcare workers, restaurant staff. The cumulative forward weight shift over an eight-hour shift in heeled shoes can be substantial.
The fix: For everyday and work wear, look for shoes with a heel drop under 8mm. Zero-drop shoes (equal heel and forefoot height) distribute weight most evenly, but transitioning too quickly from heeled to flat shoes can cause its own problems — the Achilles and calf need time to adapt. Drop incrementally if you’re making the switch.
5. Your Foot Type Creates Uneven Load Distribution
High arches, flat feet, and longer second toes all change how weight travels through the forefoot — and they all increase metatarsal stress in different ways.
High-arched feet (cavus feet) have a rigid structure that doesn’t flatten to absorb shock efficiently. More impact travels straight through the metatarsals. People with high arches tend to have pain concentrated under the first and fifth metatarsal heads.
Flat feet (low arches or overpronation) cause the foot to collapse inward during the gait cycle, shifting load to the inner metatarsals and the first MTP joint. The pain pattern is different but the mechanism is the same — concentrated pressure on a smaller area than the foot was meant to handle.
A longer second toe — what’s sometimes called a Morton’s toe — causes the second metatarsal to act as the primary weight-bearing point during push-off instead of the first. Over time, the second metatarsal head absorbs more than its share, and that’s usually where the pain develops most acutely.
The fix: This is where proper arch support (matched to your foot type, not generic) and metatarsal cushioning work together. A podiatrist can create custom orthotics for significant structural issues, but a well-fitted off-the-shelf insole handles the majority of cases.
6. Too Much Time on Hard Floors Without Adequate Cushioning
Concrete is unforgiving. The natural fat pad under your metatarsal heads — your body’s built-in shock absorber — thins with age and compresses under prolonged load. When that padding is depleted and you’re standing on concrete for eight hours in shoes with minimal cushioning, there is literally nothing left between your metatarsal heads and the floor.
This is increasingly common in office environments with polished concrete flooring, retail environments, and professional kitchens. The footwear people typically wear in these settings — smart casual shoes, kitchen clogs, fashion sneakers — often prioritize appearance over forefoot protection.
The fix: For any job requiring extended standing on hard floors, forefoot cushioning is non-negotiable. Look for shoes with a visibly thick midsole in the forefoot area, not just the heel. If your current work shoes look flat-soled from the side, that’s the first thing to change.
The Shoe Fix: What to Look For When Buying
This is the part most articles skip. Here’s what actually matters for the ball of your foot, in order of priority:
Flex point location. Do the bend test before you buy. The shoe should fold at the widest part, not the middle.
Toe box width. Enough room for all five toes to lie flat with no lateral compression. If your toes look like they’re being corralled, the box is too narrow.
Metatarsal support. Either built into the shoe or addable via insole. If you’re trying on shoes in-store, ask whether the insole is removable — if it is, you can swap in an aftermarket insole with metatarsal support.
Heel-to-toe drop. For all-day wear, under 8mm. For running with existing forefoot pain, 4–6mm is a reasonable compromise.
Forefoot cushioning thickness. Press your thumb into the forefoot area of the midsole. There should be meaningful give — not concrete-hard, not so soft your foot sinks and loses stability.
Brands that consistently do this well for forefoot comfort: Hoka (generous forefoot cushioning, wide toe box), Brooks (Adrenaline and Ghost lines work well for forefoot issues), New Balance (1080 series, excellent width options), On Running (check carefully — some models have narrow forefoot), Altra (zero drop, naturally wide toe box).
If You Only Have 10 Minutes Right Now
You don’t need to replace your shoes today to start feeling better. Here’s what you can do immediately:
Take out the insole from your current shoe. Hold it up and look at the forefoot area — is it compressed flat? Worn through? If the insole is visibly compressed under the ball of the foot, that cushioning is gone and it’s doing nothing for you. A $20–30 aftermarket insole with a metatarsal dome will make a measurable difference within days.
If the insole is fine, try this: put a thin piece of moleskin or adhesive felt pad just behind the metatarsal heads (not under them — just behind). This is a DIY metatarsal pad. It takes weight off the heads by distributing load just slightly rearward. It sounds too simple to work, but it’s the same principle as clinical metatarsal bars.
Rest, ice (10–15 minutes wrapped in a cloth, not directly on skin), and elevation at the end of the day. This won’t fix structural causes, but it reduces the acute inflammation that makes the pain worse the following morning.
What to Do If Shoe Changes Don’t Help
Give new footwear or insoles two to three weeks of consistent wear before deciding they’re not working. Your foot’s soft tissue needs time to respond to changed load distribution.
If you’ve genuinely changed your footwear, added metatarsal support, reduced time on hard floors, and the pain persists beyond three weeks — or if the pain is getting worse — see a podiatrist. This is not a “maybe if I’m really suffering” threshold. It’s a reasonable timeline.
A podiatrist can distinguish between simple metatarsalgia, Morton’s neuroma, a stress fracture (more common than most people realize, especially in runners and people who recently increased their activity), and other causes that don’t respond to conservative treatment. Leaving a stress fracture unaddressed can result in a complete break.
Go sooner if you have:
- Numbness or tingling in the toes
- Pain that wakes you up at night
- Visible swelling or bruising on the top of the foot
- Pain that started suddenly rather than gradually building
- Shooting or electric-shock sensations between specific toes
Frequently Asked Questions
Why does the ball of my foot hurt even in comfortable shoes? “Comfortable” often refers to how a shoe feels in the first 20 minutes, not how it performs over eight hours of load. The most common culprit is a shoe that lacks metatarsal support or has a flex point that doesn’t align with your foot. A shoe can feel cushioned at the heel and still be completely inadequate for forefoot support.
Why do my feet hurt after standing all day even when I’m wearing supportive shoes? Forefoot pain from prolonged standing is often about metatarsal load specifically, not overall arch support. A shoe marketed as “supportive” may have excellent longitudinal arch support with no metatarsal support at all. These are different things. Check whether your insole has any raised structure in the forefoot area — most don’t.
Is ball-of-foot pain the same as plantar fasciitis? No. Plantar fasciitis is pain in the heel and inner arch, caused by inflammation of the plantar fascia ligament. Ball-of-foot pain (metatarsalgia) affects the forefoot and is caused by metatarsal overload. They can coexist, but they have different causes and different solutions.
Why do new shoes hurt the ball of my foot? New shoes — especially leather or structured shoes — often have stiffer midsoles that haven’t compressed to your foot’s pressure pattern yet. Additionally, if the flex point of the new shoe is positioned differently from what your foot is used to, it can cause forefoot strain until you adapt. Give structured new shoes a break-in period of 1–2 weeks with limited daily wear before using them all day.
Can losing weight help with ball-of-foot pain? Yes, meaningfully. The forefoot bears 2–3 times body weight during walking, so even a modest reduction in body weight reduces forefoot load significantly. That said, this is a long-term factor — if you’re in pain now, shoe changes will provide faster relief.
Why does only one foot hurt in the ball? Asymmetric forefoot pain is often caused by a structural difference between the two feet — different arch heights, a longer second toe on one side, or a previous injury that changed your gait. It’s also worth checking whether you have different wear patterns on the soles of your shoes — one sole worn more on the inner forefoot suggests overpronation on that side.
Should I use a metatarsal pad or a full insole? If your pain is localized to the ball of the foot with no other complaints, a metatarsal pad or dome is often sufficient and more targeted. A full insole with metatarsal support is better if you also have arch discomfort or if you overpronate. Many people find that trying the pad first (cheap and quick) gives them useful information about whether metatarsal offloading is the issue before committing to a full insole.
The Bottom Line
Ball-of-foot pain is common, uncomfortable, and — in most cases — genuinely solvable without a medical appointment. The shoe you’re wearing is almost always part of the equation, whether that means the flex point is wrong, the toe box is too narrow, the heel drop is shifting load forward, or the forefoot cushioning has long since given up.
Start with the shoes. Do the bend test. Check the toe box. Consider a metatarsal insole. Give it two to three weeks. Most people who do this systematically find that the problem either resolves or becomes clear enough to explain to a doctor efficiently.
If you’re dealing with forefoot pain and thinking about your next shoe purchase, read our guide on what to look for in a walking shoe — it covers flex points, heel drop, and forefoot construction in detail with specific model recommendations. Or if you’re a nurse, retail worker, or anyone spending long shifts on hard floors, our piece on what feet that stand all day actually need from a shoe is written specifically for that situation.
References
- Espinosa, N., & Brodsky, J.W. “Metatarsalgia.” Journal of the American Academy of Orthopaedic Surgeons, 2010.
- Garbalosa, J.C., et al. “The frontal plane relationship of the forefoot to the rearfoot in an asymptomatic population.” Journal of Orthopaedic & Sports Physical Therapy, 1994.
- Kernozek, T.W., & Zimmer, K.A. “Footwear effects on plantar pressure distribution and walking kinematics in older adults.” Gait & Posture, 2000.
- Mickle, K.J., et al. “Foot pain, plantar pressures, and falls in older people: a prospective study.” Journal of the American Geriatrics Society, 2010.
- American Podiatric Medical Association (APMA). Metatarsalgia. apma.org
- Tong, J.W., & Kong, P.W. “Association between foot type and lower extremity injuries: systematic literature review with meta-analysis.” Journal of Orthopaedic & Sports Physical Therapy, 2013.